
The 1 Effortless Way To Differentiate Between Meniere’s Disease and BPPV


Vestibular disorders can be frustrating and complex, but they are all actually incredibly different. There are a few key factors that differentiate each from one another very distinctly. Two very distinct, but often confused, diagnoses are BPPV and Meniere’s Disease. Remember, BPPV stands for Benign Paroxysmal Positional Vertigo. The differences lie in the diagnostic criteria, as well as the clinical presentations. Both do come with room-spinning vertigo, but they will feel very very different.
Diagnostic Criteria
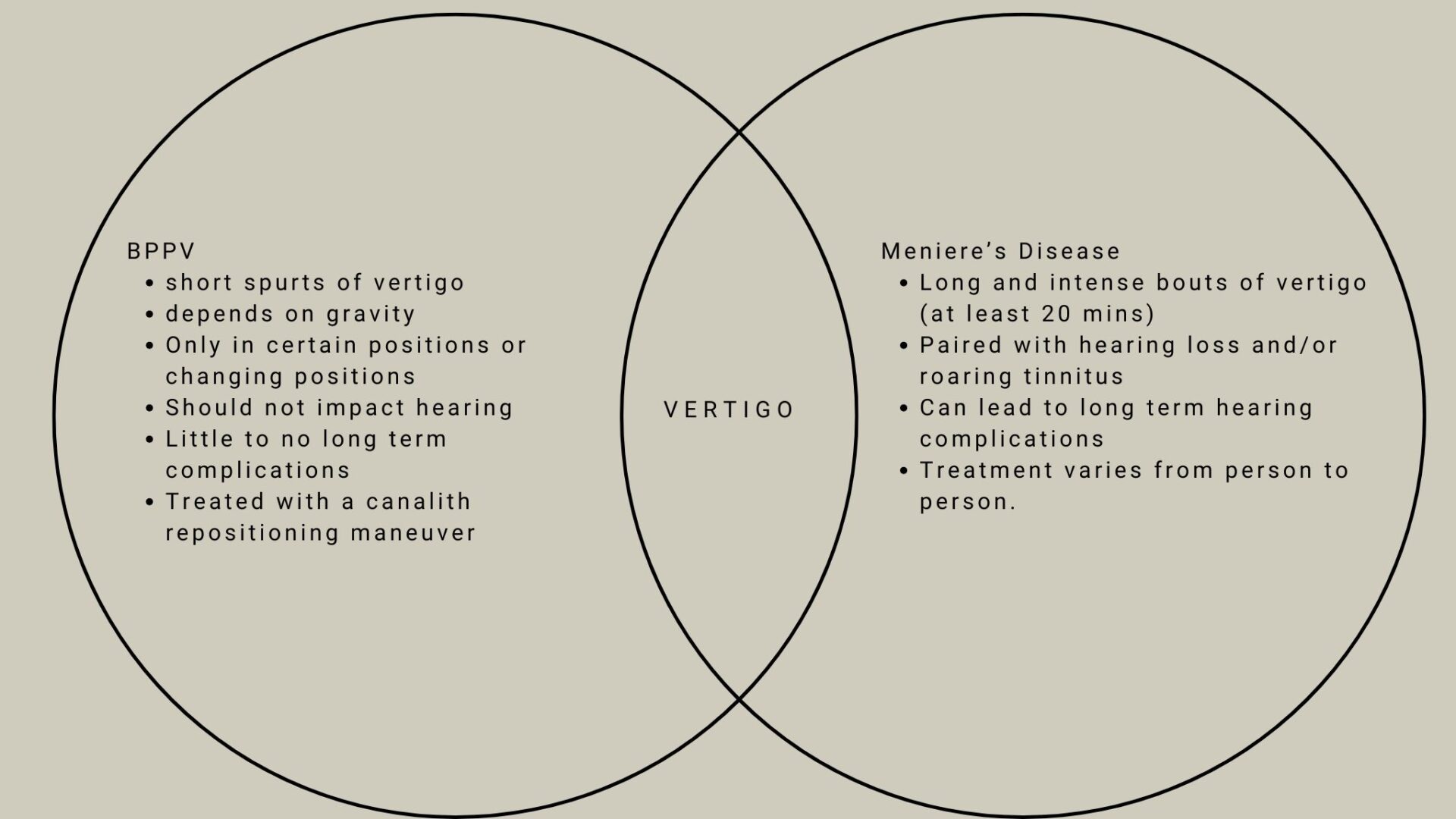
These two diagnoses are very different. BPPV will cause short and spontaneous episodes of vertigo, while Meniere’s Disease triggers long and difficult to tolerate episodes of vertigo.
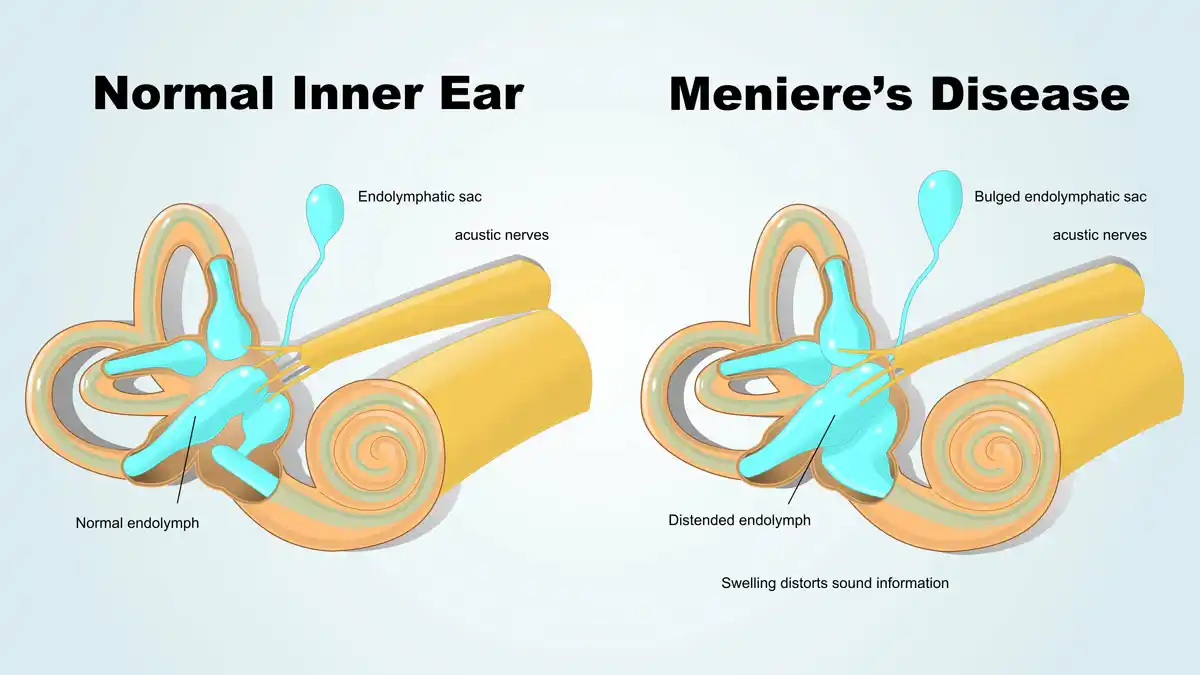
Meniere’s Disease (MD) Diagnostic Criteria:
- Two or more spontaneous episodes of vertigo each lasting 20 minutes to 12 hours
- Audiometrically documented low- to medium frequency sensorineural hearing loss in one ear, defining the affected ear on at least one occasion before, during or after one of the episodes of vertigo
- Fluctuating aural symptoms (hearing, tinnitus, or fullness) in the affected ear
- Not better accounted for by another vestibular diagnosis (1)
This is important to understand because many people (and providers) diagnose Meniere’s Disease despite people not actually meeting these criteria. This is especially try of my patients who tell me they have MD but have never experienced room spinning vertigo, or they experience quick spins, rather than long duration spinning, but still have an MD diagnosis. Those things do not qualify you for an MD diagnosis. So, when you may be thinking you may have this diagnosis, know that is both rare and requires a LOT of room spinning vertigo.
Speaking of being rare, yes, Meniere’s Disease is really rare. According to the American Hearing Research Foundation, only about .2% of the US population has Meniere’s Disease, where as BPPV is much more common (2). BPPV has a lifetime prevalence of 2.4%, meaning it will happen in about 2.4 % of the population at some point in their in their lifetime. That is WAY more than Meniere’s Disease (3)!
Benign Paroxysmal Positional Vertigo Diagnostic Criteria
A. Recurrent attacks of positional vertigo or positional dizziness provoked by lying down or
turning over in the supine position.
B. Duration of attacks < 1 min.
C. Positional nystagmus elicited after a latency of one or few seconds by the Dix-Hallpike maneuver or side-lying maneuver (Semont diagnostic maneuver). The nystagmus is a combination of torsional nystagmus with the upper pole of the eyes beating toward the lower ear combined with vertical nystagmus beating upward (toward the forehead) typically lasting < 1 minute.
D. Not attributable to another disorder.
Okay let’s break these down, because they’re a bit more confusing than the Meniere’s Disease diagnostic criteria.
What the BPPV criteria are saying is that when you lie down and sit up, you will have spontaneous room-spinning vertigo for less than 1 minute, which also has a delay (typically 5-10s) because it sets. AND it needs to be non-attributable to another disorder. This is where things get sticky, because vestibular migraine can actually act JUST like BPPV. I see people almost weekly in my clinic that say ‘I have been doing BPPV maneuvers for weeks, and NOTHING is happening,’ and it’s almost always actually vestibular migraine. To learn about the differences between vestibular migraine and BPPV, please click here.
So, how do I know the difference Between Meniere’s Disease and BPPV?
The best, and easiest, way to know the difference is based upon the length of your room spinning vertigo. If your vertigo is quick, and ends in less than a minute, it’s more likely to be BPPV (unless, of course, it’s VM, please read here). If the vertigo is more arduous, tiring, lasting longer than 20 minutes, but also causing hearing loss and tinnitus, it’s more likely to be Meniere’s disease.
What do I do if I have BPPV or Meniere’s Disease?
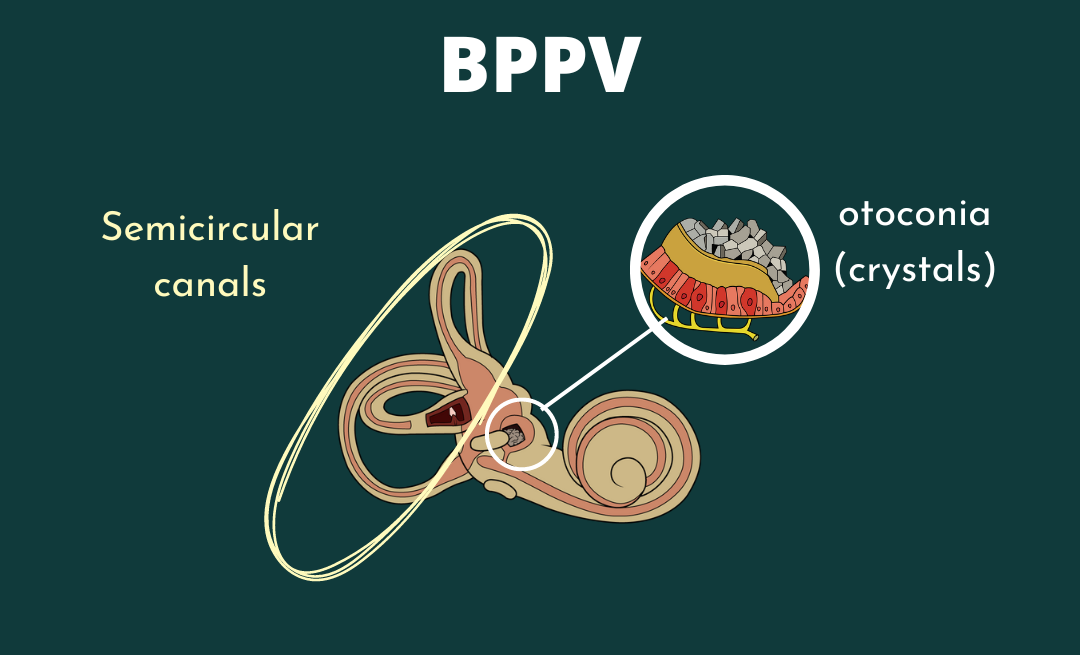
If you have BPPV, the best plan of care is to call your local physical therapist (hopefully a vestibular therapist!) and get in for a canalith repositioning maneuver to move the crystals back to where they belong! Out of your semicircular canals, and into the otolith organs.
If you have Meniere’s Disease, be sure to call your local vestibular ENT to talk about your treatment options and look further into why your body may have triggered this. There are definitely treatment options for you!
No matter what, there are treatment options for BPPV, MD, and VM. We have treatment options in Vestibular Group Fit, or you can find them at your local doctor. Be sure to address: the actual disorder, inflammation, lifestyle, blood work, and more! If you have questions about what these things should be, please reach out and join us here!
Sources:
(1) American Academy of Audiology. (2022, January 14). Classifications of meniere’s disease. https://www.audiology.org/classifications-of-menieres-disease/
(2) Meniere’s disease. American Hearing Research Foundation. (2022, August 24). https://www.american-hearing.org/disease/menieres-disease/
(3) von Brevern M, Radtke A, Lezius F, Feldmann M, Ziese T, Lempert T, Neuhauser H. Epidemiology of benign paroxysmal positional vertigo: a population based study. J Neurol Neurosurg Psychiatry. 2007 Jul;78(7):710-5. doi: 10.1136/jnnp.2006.100420. Epub 2006 Nov 29. PMID: 17135456; PMCID: PMC2117684.

Latest articles