
How Hormones Impact Vestibular Conditions


Hormones and Vestibular Conditions
Hormones are the chemical messengers for our body that travel through our bloodstream. They are in charge of so many of our bodily functions: hunger, emotions, growth and development, feeling ill etc. Research has shown a hormonal connection to the vestibular system and certain vestibular conditions. In this article we will look at estrogen’s and prolactin’s role in vestibular conditions. (1)
Estrogen is present in all humans but there are higher levels of estrogen in females. During childbearing years for females, estrogen levels change monthly throughout the menstrual cycle.
Estrogen levels drop 2 days before one’s period and right before ovulation; in between those drops there is a gradual rise in estrogen levels. The drop is estrogen during ovulation and before your period is when most people notice an increase in vestibular symptoms. (2)
Prolactin has over 300 roles but today we’re looking at its involvement with milk production and breastfeeding after childbirth. This hormone is controlled by the hypothalamus, and in some theories the hypothalamus plays a role in migraine. Based on the theories including the hypothalamus in migraine, prolactin could play a role in migraine in those who are breastfeeding. (3)
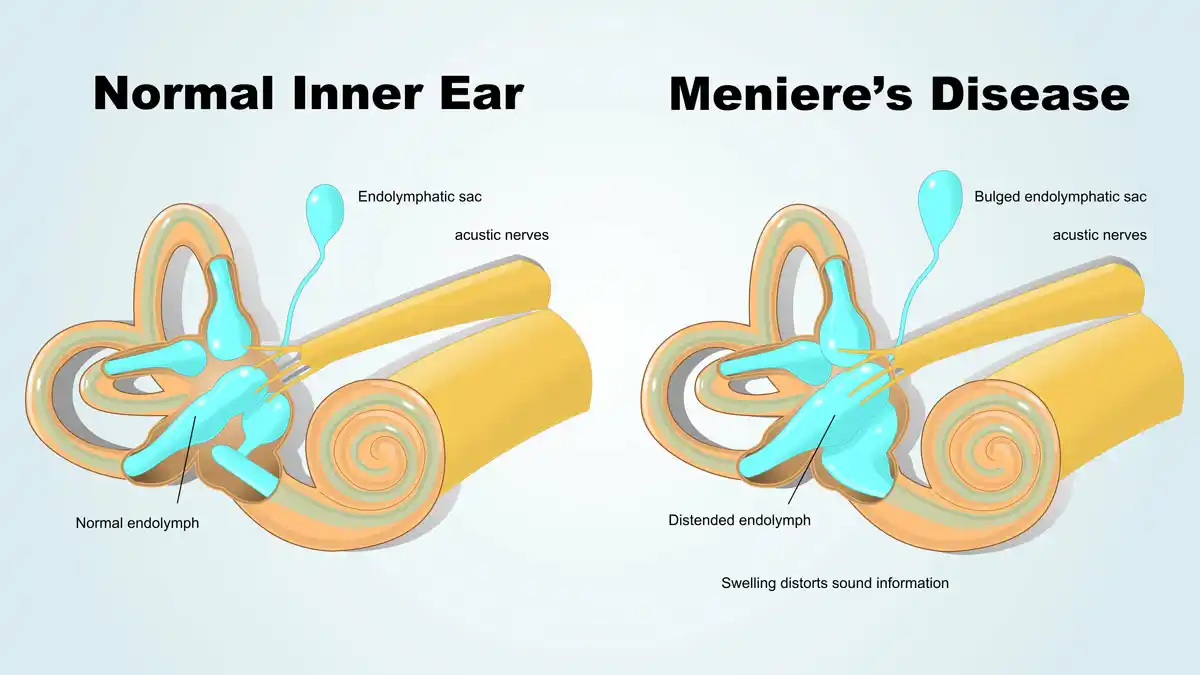
Meniere’s disease and Hormones
Common hormonal changes impacting Meniere’s disease are during the premenstrual phase of your period and pregnancy. Hormonal changes and fluid retention during these times can increase attacks. Fluid retention and hormonal changes can result in a change in fluid movement that can result in a Meniere’s attack. Research showed in one trial that those who had hormone therapy found some benefit in reducing the number of attacks. (4)
Acoustic neuroma and Hormones
Acoustic neuroma is a slow growing mass that impacts the vestibulocochlear nerve. This mass is typically benign and can cause imbalance, dizziness and hearing changes.
A study in mice showed increased growth of acoustic neuroma tissue. It appears that estrogen affects the pace of mass growth in acoustic neuroma. (5) Acoustic neuroma is also more common in women than in men, this may be in part due to higher estrogen levels in women, but more information and research is needed.
Vestibular migraine and Hormones
Migraine in general can be linked to hormonal fluctuations leading up to or at the start of one’s period (6,7). For vestibular migraine this may increase dizziness. The sudden drop in estrogen during menstruation and ovulation can cause an exacerbation of vestibular migraine. It’s been shown that migraineurs have a faster drop in estrogen than non migraineurs. (7,8). Another theory regarding migraine involves the relationship between estrogen and serotonin. Estrogen impacts serotonin, serotonin impacts the trigeminal nerve. The trigeminal nerve can cause migraines due to its release of CGRP. CGRP has been connect to migraine and the reduced ability to process CGRP, and anti-CGRP medicines were created to help treat migraines. (8)
Prolactin can also play a role in migraine. Both individuals with higher and lower levels of prolactin have been correlated with various types of migraines. Prolactin also has a connection to the trigeminal nerve and hypothalamus which have been theorized to have roles in migraines. (9). Prolactin has so many functions day to day so just a reminder that you don’t have to be breastfeeding for prolactin to have an influence on migraines. Breastfeeding is one of the many jobs prolactin is involved in, so if you’re breast feeding and notice changes, prolactin could be playing a role.
A side note: If you experience more headache symptoms with your migraine, research has shown addressing low testosterone (increase to higher levels within normal range) has been shown to reduce headache frequency. (10)
Managing hormonal changes
Hormone therapy is one way to address hormonal changes. This is a discussion to have with your doctor to see if this is a right fit for you. Hormone testing is generally not accurate because our hormone levels are always changing. Most hormone therapy involved dosing bioidentical hormones to help smooth out the fluctuations. This can be prescribed as a pill, patch, IUD or gel. (18/19). Some find hormone therapy helpful, others find that it makes symptoms worse, talk to your doctor about starting hormone therapy and give them updates on how your feeling so they can adjust your plan.
Other options to consider if hormone therapy isn’t for you are:
- Triptans: talk to your doctor if triptans could work for you and for your doctor to create and monitor your plan.
- Preventative medications: another great conversation for your doctor!
- Talk to your doctor about preventative supplements
- Magnesium
- Riboflavin (b2)
- Coq10
- Vitamin D
- Omega 3s
- GammaCore or Cefaly to assist with nerve stimulation for symptoms. (11)
Stay tuned for the breakdown of hormones throughout the different phases of life (puberty, pregnancy, post partum, peri/menopause) in our next article!
Do you want to learn more about how hormones can impact your vestibular condition?
Click here to Learn How to Manage Your Hormones & Vestibular Disorder
Disclaimer:
Remember: this post is for informational purposes only and may not be the best fit for you and your personal situation. It shall not be construed as medical advice. The information and education provided here is not intended or implied to supplement or replace professional medical treatment, advice, and/or diagnosis. Always check with your own physician or medical professional before trying or implementing any information read here.
Resources
- Kesserwani, H. (2021). Migraine triggers: An overview of the pharmacology, biochemistry, atmospherics, and their effects on Neural Networks. Cureus. https://doi.org/10.7759/cureus.14243
- Bb Natural Health. (2018, October 11). Cravings during your cycle. BB Natural Health. Retrieved April 21, 2022, from https://www.bbnaturalhealth.co.za/blogs/articles/91631363-cravings-during-your-cycle
- Tzabazis A, Kori S, Mechanic J, Miller J, Pascual C, Manering N, Carson D, Klukinov M, Spierings E, Jacobs D, Cuellar J, Frey WH 2nd, Hanson L, Angst M, Yeomans DC. Oxytocin and Migraine Headache. Headache. 2017 May;57 Suppl 2:64-75. doi: 10.1111/head.13082. PMID: 28485846.
- Andrews JC, Ator GA, Honrubia V. The Exacerbation of Symptoms in Meniere’s Disease During the Premenstrual Period. Arch Otolaryngol Head Neck Surg. 1992;118(1):74–78. doi:10.1001/archotol.1992.01880010078020
- Stidham KR, Roberson JB Jr. “Effects of Estrogen and Tamoxifen on Growth of Human Vestibular Schwannomas in the Nude Mouse.” Otolaryngology— Head and Neck Surgery, 120(2):262–264, 1999
- SD;, S. (n.d.). Sex hormones and headache. Revue neurologique. Retrieved April 21, 2022, from https://pubmed.ncbi.nlm.nih.gov/11139745/
- World Migraine Summit. (2022). How Women’s Hormones Affect Migraine. Retrieved April 2022.
- Northrup, Christiane. (2015, May 29). Migraines. Christiane Northrup, M.D. Retrieved April 21, 2022, from https://www.drnorthrup.com/migraines/
- Gazerani, P. (2021, September 24). A link between migraine and prolactin … – future-science.com. future-science.com. Retrieved April 22, 2022, from https://www.future-science.com/doi/10.2144/fsoa-2021-0047
- Watson, S. (2020, July 7). Low T and headaches: What’s the connection? Healthline. Retrieved April 21, 2022, from https://www.healthline.com/health/low-testosterone/headache
- Beh, Shin C . Victory Over Vestibular Migraine: The ACTION Plan for Healing & Getting Your Life Back (p. 229). Beh Center for Vestibular & Migraine Disorders, PLLC. Kindle Edition.


