BPPV and Vestibular Migraine: 4 ways to master the difference
In Vestibular Group Fit, Dr Madison Oak and Vestibular PT Cheryl Wylie, MPT talk all things BPPV and vestibular migraine. They discuss what BPPV is, what assessment and treatment look like, and Cheryl’s amazing app Healing Vertigo (check it out here). There’s great conversation too revolving around a very common yet difficult task, am I dizzy with a vestibular migraine flare, or BPPV? Read on for some background, or jump to the differences between BPPV and VM at the of this post.
Cheryl Wylie has been working in vestibular rehabilation for 13 years. Throughout her time traveling, she realized how common BPPV is, yet how difficult it can be to get it treated for those outside of big cities and specialized therapists. The app Cheryl created, Healing Vertigo, is designed for patients to learn how to address BPPV themselves.
What is BPPV?
BPPV stands for “Benign Paroxysmal Positional Vertigo”. This is a common vestibular condition, and gets its name from its own characteristics.
Benign: Not harmful (Don’t worry, we know firsthand how disruptive, scary and down right uncomfortable BPPV is…we have had it! They used the term benign in naming BPPV due to the fact it is not considered life threatening.)
Paroxysmal: sudden onset
Positional: certain head/body positions bring on symptoms
Vertigo: sensation of motion or spinning
BPPV and the Vestibular System
We’ll keep this review brief, but feel free to check out this previous post that dives deep into all things BPPV here.
Our vestibular system has 3 semicircular canals. These canals are filled with fluid and sit at different angles. Their job is to detect angular motion (are we moving sideways, up, down diagonal).
In the otolith of the inner ear, tiny (but heavy for their size) crystals that help detect gravity and motion.
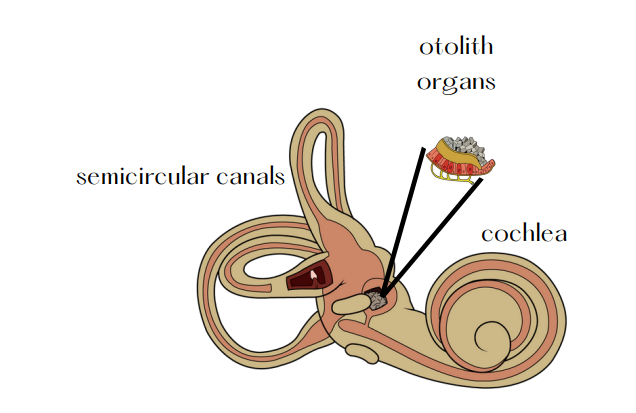
If a crystal breaks away from the otolith and finds it’s way into a semicircular canal, this is the start of BPPV. When this crystal moves through the semicircular canal, the crystal pushes the fluid of the canal at a different rate. Our inner ear is now sending two very different signals of movement to our brain to try and understand. This results in a specific eye movement called a nystagmus (more on this here). This is why testing involves certain head positions, and looking at your eyes to assess any nystagmus present. Nystagmus is important information in addition to head position to know the next course of action, treatment! Here’s a chart of the different nystagmus here.
NOT EVERYONE GETS DIZZY WITH BPPV. Some may not feel dizzy with BPPV, but off balance. This is why it’s important to screen for BPPV in those that are dizzy and those with balance concerns to rule out BPPV.
Vestibular Migraine
Vestibular migraine is a neurological condition that can result in a variety of unpleasant symptoms. Common symptoms of vestibular migraine include: brain fog, light/sound sensitivity, neck pain, tingling, vision changes, and dizziness and/or vertigo. For more background check out our beginners guide to vestibular migraine.
Those with vestibular migraine have most likely been treated for BPPV. The kicker here though, is not all had BPPV. Unfortunately, this results in people getting treated for BPPV over and over, with no change in symptoms or feeling worse than before. This is because vestibular migraine can result in positional dizziness, but is not due to BPPV. This is why it’s important to understand the mechanism and nystagmus of BPPV to determine if treatment is warranted, or if it is due to a vestibular migraine attack.
BPPV and Vestibular Migraine, which is it?
BPPV charactersistics:
- lasts 10-30 seconds typically (but can last longer if you have cupulolithiasis-read on here)
- nystagmus that matches a semicircular canal (chart here)
- Tends to have a slight symptom delay (a few seconds)
- will continue to happen until treated (spontaneous resolution can occur, but can take weeks and isn’t guaranteed)
Vestibular migraine characteristics:
- quick spins while sitting up or sensation of dropping
- nystagmus isn’t consistent. or doesn’t match that of BPPV
- comes with a migraine attack (light/sound/smell sensitivity etc).
- You feel like you keep doing the Epley and it doesn’t work
- You get episodes of spinning or dizziness in certain positions but will go away in a day or two without you doing any treatment and just “wait it out”.
It’s hard to know the difference between BPPV and vestibluar migraine. Hopefully this list helps point you in the right direction. BPPV needs to be treated with a repositioning maneuver to improve. A vestibular migraine needs to be treated during a flare, and then work on managing symptoms and increasing your migraine threshold. If you’re unsure, schedule with your vestibular PT for an assessment for BPPV or check out Cheryl’s Healing Vertigo App (website here, video presentation here)
Disclaimer
Want to learn more about what to expect with BPPV assessment and treatment, debu7nking BPPV myths, reducing BPPV risk and other vestibular tools from the experts and be a part of a supportive community to get back to your daily life? Find out more at this link: https://thevertigodoctor.com/about-group/
Disclaimer:
Remember: this post is for informational purposes only and may not be the best fit for you and your personal situation. It shall not be construed as medical advice. The information and education provided here is not intended or implied to supplement or replace professional medical treatment, advice, and/or diagnosis. Always check with your own physician or medical professional before trying or implementing any information read here.
